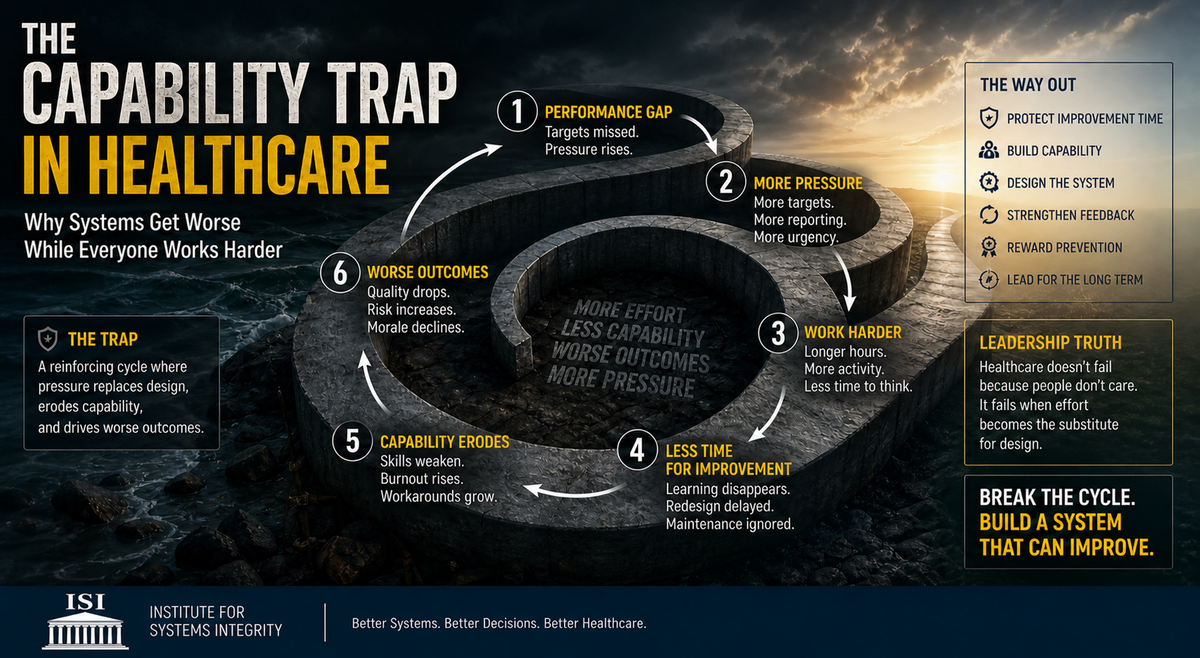
The Capability Trap in Healthcare Why Systems Get Worse While Everyone Works Harder
Healthcare does not fail because people lack effort. It fails when effort substitutes for system design. The capability trap reveals how increasing pressure erodes capacity, weakens performance, and creates a self-reinforcing cycle of decline
Dr Alwin Tan, GAICD, MBBS, FRACS, EMBA (Melbourne Business School)
Senior Surgeon | Governance Leader | HealthTech Co-founder |
Harvard Medical School — AI in Healthcare |
Australian Institute of Company Directors — GAICD graduate|
University of Oxford — Sustainable Enterprise
An Institute for Systems Integrity (ISI) Perspective
Executive summary
Healthcare systems rarely fail from lack of effort.
They fail when effort becomes the substitute for system design.
The capability trap describes a reinforcing dynamic in which leaders respond to performance pressure by increasing workload and urgency, while unintentionally reducing the time and capacity required for improvement. This leads to declining capability, worsening performance, and escalating pressure — a cycle that can persist despite high commitment and visible activity.
For boards and executives, this is not an operational inconvenience.
It is a governance risk.
1. The hidden nature of system decline
Healthcare organisations are rarely idle.
They are busy, responsive, and often deeply committed to delivering care under pressure.
Yet beneath this activity, a quieter dynamic may be unfolding:
- Improvement work is deferred
- Training is reduced
- Reflection disappears
- Workarounds become normal
- Staff fatigue accumulates
- Learning weakens
From the outside, the system appears functional.
From the inside, its capability is eroding.
This is the central paradox:
The system appears to work because people are compensating for its design weaknesses.
2. Understanding the capability trap
The capability trap, first described in system dynamics literature, explains how short-term responses to performance pressure can undermine long-term system performance (Repenning and Sterman, 2002).
The dynamic can be summarised as follows:
Performance gap emerges
↓
Leadership increases pressure
↓
Teams work harder
↓
Time for improvement is displaced
↓
Capability erodes
↓
Performance worsens
↓
Pressure increases further
This is not a linear problem.
It is a reinforcing loop.
And like many reinforcing loops, it is difficult to detect early because initial responses may appear effective.
3. Why healthcare is structurally vulnerable
Healthcare operates under conditions that amplify this risk:
- Demand is continuous and unpredictable
- The moral cost of delay is high
- Systems cannot easily pause for redesign
- Workforce capacity is finite
- Complexity is inherent
When demand exceeds capacity, people compensate.
They extend effort.
They adapt locally.
They protect patients.
Over time, this creates a dangerous illusion:
That the system is functioning — when in reality it is being held together by human effort.
This effort is not sustainable.
Nor is it visible in most governance frameworks.
4. The short-term success problem
One of the reasons capability traps persist is that pressure often works — temporarily.
In the short term, increased effort can:
- Reduce backlogs
- Improve throughput
- Meet targets
- Contain crises
These outcomes reinforce the belief that pressure is effective.
However, the longer-term effects are different:
- Capability is not replenished
- Learning is deferred
- Risk accumulates
- Performance becomes more fragile
As Sterman (2001) notes, interventions in complex systems often produce delayed and counterintuitive effects.
Short-term success may therefore mask long-term decline.
5. The governance blind spot
Boards typically monitor performance indicators such as:
- Activity
- Throughput
- Financial metrics
- Compliance
- Target achievement
What is less visible is capability:
- Time allocated to improvement
- Workforce learning and development
- Maintenance of systems and processes
- Psychological safety
- Quality of feedback loops
- Reliance on workarounds
This creates a governance blind spot.
A system may appear to improve while its underlying capacity to sustain performance is weakening.
The updated Medical Research Council framework for complex interventions emphasises the importance of understanding system interactions, context, and implementation dynamics — not just outcomes (Skivington et al., 2021).
For governance, this means:
Performance must be interpreted alongside capability.
6. Attribution error and misdiagnosis
When performance declines, organisations often default to individual explanations:
- Staff are not working hard enough
- Managers are not driving performance
- Teams lack accountability
- Culture is weak
This is a form of attribution error.
Repenning and Sterman (2002) describe how organisations can misinterpret system-generated outcomes as failures of individual effort, leading to further pressure that exacerbates the problem.
In healthcare, this creates a harmful cycle:
- System overload →
- Staff compensate →
- Capability erodes →
- Performance declines →
- Individuals are blamed →
- Pressure increases →
- System deteriorates further
This is not effective accountability.
It is systemic misdiagnosis.
7. Productive versus destructive pressure
Pressure is not inherently harmful.
In certain contexts, it is necessary.
Productive pressure
- Time-limited
- Clearly defined objectives
- Supported by additional resources
- Followed by recovery and learning
- Used to manage acute risk
Destructive pressure
- Chronic and sustained
- Substitutes for redesign
- Crowds out improvement
- Suppresses feedback
- Normalises overwork
- Erodes capability
The distinction is critical.
Resilient systems use pressure strategically.
Fragile systems depend on it continuously.
8. The ISI capability framework
From a systems-integrity perspective, the capability trap can be understood as a failure to balance:
- Delivery capacity (what the system produces today)
- Improvement capacity (what the system can become tomorrow)
When delivery consistently crowds out improvement, decline becomes inevitable.
Key signals of capability erosion
- Rising reliance on workarounds
- Increasing burnout and turnover
- Declining time for training and supervision
- Repeated incidents without systemic resolution
- Reduced openness in reporting concerns
- Growing gap between targets and lived reality
These are not soft signals.
They are early warnings of system instability.
9. Escaping the capability trap
Breaking the trap requires deliberate governance action.
1. Protect improvement capacity
Improvement must be structurally protected, not opportunistic.
2. Make capability visible
Boards should track capability indicators alongside performance.
3. Separate surge from normal operations
Emergency response should not define standard operating practice.
4. Accept temporary performance dips
System redesign requires time and may initially reduce output.
5. Strengthen feedback loops
Decisions must be informed by real operational signals.
6. Reframe accountability
Accountability must extend to system design, not only individual performance.
7. Reward prevention
Prevented failures must be recognised as outcomes, not absences.
10. ISI position
The capability trap represents a structural governance risk across healthcare systems.
It affects:
- Patient safety
- Workforce sustainability
- Clinical outcomes
- Organisational resilience
- Financial performance
- Innovation capacity
A system that relies on sustained over-effort is not robust.
It is operating beyond its designed limits.
And when such systems fail, they often do so abruptly.
Conclusion
Healthcare systems do not collapse because people stop trying.
They collapse because effort is used to sustain performance in systems that are no longer capable of improving.
The capability trap begins when leaders attempt to close performance gaps by increasing pressure while reducing the system’s ability to learn.
The result is predictable:
More effort.
Less capability.
Worse outcomes.
From a governance perspective, the question is not:
“Are we meeting our targets?”
The real question is:
“Are we building a system that can continue to perform — without exhausting the people holding it together?”
References (Harvard style)
Belrhiti, Z., Damme, W.V., Belalia, A. and Marchal, B. (2018) ‘Complex leadership in healthcare: A scoping review’, International Journal of Health Policy and Management, 7(12), pp. 1073–1084.
Repenning, N.P. and Sterman, J.D. (2002) ‘Capability traps and self-confirming attribution errors in the dynamics of process improvement’, Administrative Science Quarterly, 47(2), pp. 265–295.
Skivington, K. et al. (2021) ‘A new framework for developing and evaluating complex interventions: Update of Medical Research Council guidance’, BMJ, 374, n2061.
Sterman, J.D. (2001) ‘System dynamics modeling: Tools for learning in a complex world’, California Management Review, 43(4), pp. 8–25.